 Facebook
Facebook  Twitter
Twitter  Soundcloud
Soundcloud  Youtube
Youtube  Rss
Rss 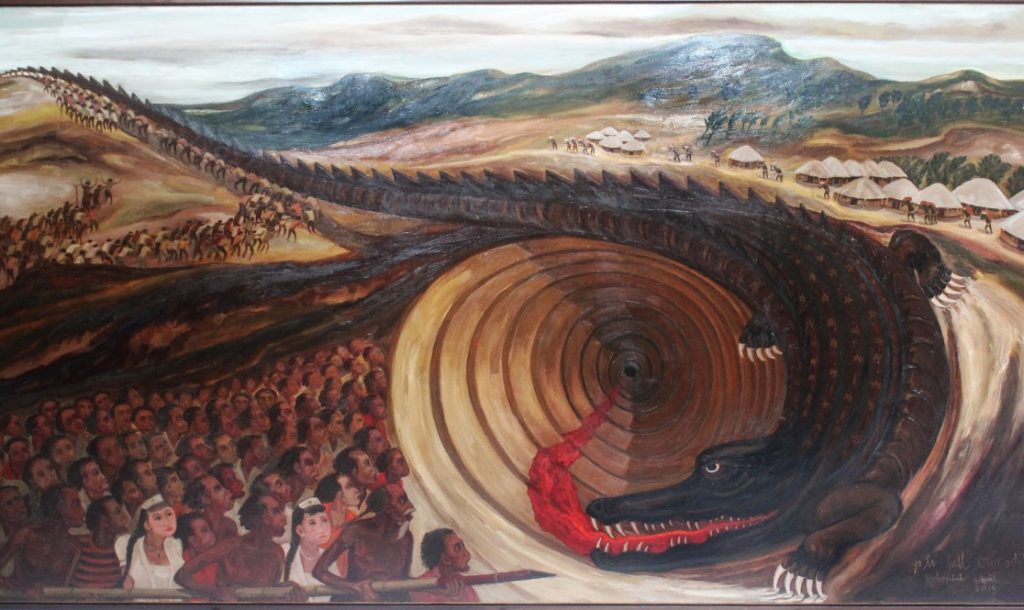
Mark Micale and Hans Pols, eds. Traumatic Pasts in Asia: History, Psychiatry, and Trauma, 1930 to the Present. New York: Berghahn, 2021.
You can also read a review of the same book, by Jason Crouthamel, on New Mandala here.
How did this book come about? Both of us are historians of psychiatry, and we frequently met at conferences when Hans was living in North America. One of most fascinating topics in the history of psychiatry is the appearance, increasing popularity, and disappearance of psychiatric diagnoses over time. Mark has written about the history of hysteria —once commonly diagnosed, now rarely identified. After moving to Sydney, Australia, some 20 years ago, Hans became interested in [link] psychiatry and mental health care in Indonesia—its past, present state, and future. In Indonesia, not surprisingly, psychiatry looks somewhat different. It is not possible to transplant North American theories and treatments to clinical presentations in other parts of the world without modification and adaptation.
Today, one of the most widely used diagnostic categories in psychiatry is Posttraumatic Stress Disorder (PTSD). It was officially recognised by the American Psychiatric Association in 1980, when it was included in the third edition of its authoritative Diagnostic and Statistical Manual of Mental Disorders (DSM-III), nicknamed the “Bible of Psychiatry.” PTSD captures the psychological after-effects experienced by individuals who have been exposed to extreme violence or catastrophic events “outside the realm of normal human experience.” These include bombing, torture, death camps, military combat, physical or sexual assault, and natural disasters. Initially, the PTSD diagnosis was primarily applied to Vietnam veterans, Holocaust survivors, and women who had suffered domestic and sexual abuse.
The concept of PTSD has various uses within psychiatry. But trauma and PTSD often appear in discussions of non-psychiatrists and non-physicians as well. As historians, we view debates about trauma as ways to cast light on violence and horrific experiences—how they come about, their nature, and what can be done about them. These debates are socially, culturally, and politically highly significant.
Before the publication of DSM-III, psychiatrists and others used a range of terms to describe the psychological effects of war and severe accidents. These included shellshock, war neurosis, railway spine, combat fatigue, and combat stress. In 2001, Mark co-edited an influential volume on this topic with Paul Lerner and noted that many of these diagnostic categories fell in and out of favour over time. In contrast, PTSD’s popularity in the Western world has steadily increased. According to some critics, PTSD is now ubiquitous in Western society. According to these critics, the condition is increasingly diagnosed in individuals who have experienced less severe traumas, thereby potentially trivialising the diagnosis.
Hans and Mark met again in 2017, when Mark was invited by the University of Newcastle, Australia, for a 2-month visit. Over several beers, Hans convinced Mark that Traumatic Pasts deserved a sequel focusing on the non-Western world. Because of Hans’ work in Indonesia and his familiarity with the history of psychiatry and mental health in Asia, he suggested co-editing a volume focusing on Asia. Traumatic Pasts in Asia is the outcome.
Traumatising events are not unique to the West. People in Asia have been repeatedly exposed to deeply traumatic events including military violence and occupation, civil war, torture, terrorism, and acts of genocide, as well as natural disasters such as volcanic eruptions, tropical storms, floods (including the 2004 Indian Ocean tsunami), earthquakes, and prolonged droughts. Critics of Western and global psychiatry have argued that Western diagnostic categories, in particular PTSD, do not adequately capture the way people in the rest of the world react to severe trauma.
The contributors to Traumatic Pasts in Asia investigate how people in Asia have reacted to traumatising events by rebuilding their communities and by developing individual and collective repertoires to overcome trauma, regain a sense of equilibrium, and foster resilience. They focus on how they found ways of rebuilding their communities and their sense of self. Some contributors have focused on the extent to which Western diagnostic categories have influenced the ideas and approaches of local health personnel. Others analyse the way people in Asia have dealt with traumatic events without resorting to medical theories and approaches.
The chapters in the book are written by historians and anthropologists—a fruitful combination, because combining approaches from both disciplines leads to unusually good insights. The volume’s historians have analysed trauma-related diagnostic categories over time, while its anthropologists have investigated the unique features of how people in various Asian contexts react to traumatic events.
If he’s serious about building Indonesia’s “human capital”, Jokowi should make mental health a policy priority.
Mental health care in Indonesia: short on supply, short on demand
Traumatic Pasts in Asia contains historical chapters on Japan, Taiwan, Korea, and Vietnam. Eri Nakamura analyses how German ideas on trauma influenced Japanese military psychiatry during World War II. Even though psychiatrists publicly denied that soldiers of the Imperial Army could succumb to trauma, they still identified soldiers who had broken down. Before World War II, as Harry Wu describes, Japanese physicians investigated the psychological after-effects of a volcanic eruption in Taiwan—long before natural disasters became of interest of psychiatrists elsewhere. Ran Zwigenberg investigates the complete absence of research on the trauma among atomic bomb survivors in Hiroshima and Nagasaki in post-war Japan. Even though these individuals were obvious candidates for this kind of research, it was never conducted, for various political reasons.
Jennifer Yum-Park analyses the enthusiastic reception of American approaches to war neurosis and combat stress (“Yankee-style trauma”) among Korean physicians during the Korean war. In a path-breaking essay, Narquis Barak investigates the reactions of Vietnamese psychiatrists and physicians during the Vietnamese War (called the American war in Vietnam). Up to this day, Vietnamese psychiatrists argue that there is no PTSD in Vietnam. Neither the Korean nor the Vietnamese story have been told before.
Vannessa Hearman focuses on the exchange of letters between a female political prisoner in Suharto’s Indonesia and a British woman Quaker. These letters provided the only source of contact with the outside world for this prisoner and helped her to survive. Dyah Pitaloka and Mohan J. Dutta investigate the performances of the Indonesian Dialita choir. Its members are women who survived the horrors of the aftermath of Suharto’s coup in 1965. In their performances, they sing songs of hope and resilience, and thereby connect to younger audiences. Neither chapter focuses on medical or psychiatric conceptions of trauma. Instead, it focuses on rituals and practices people use to deal with traumatic pasts and presents.
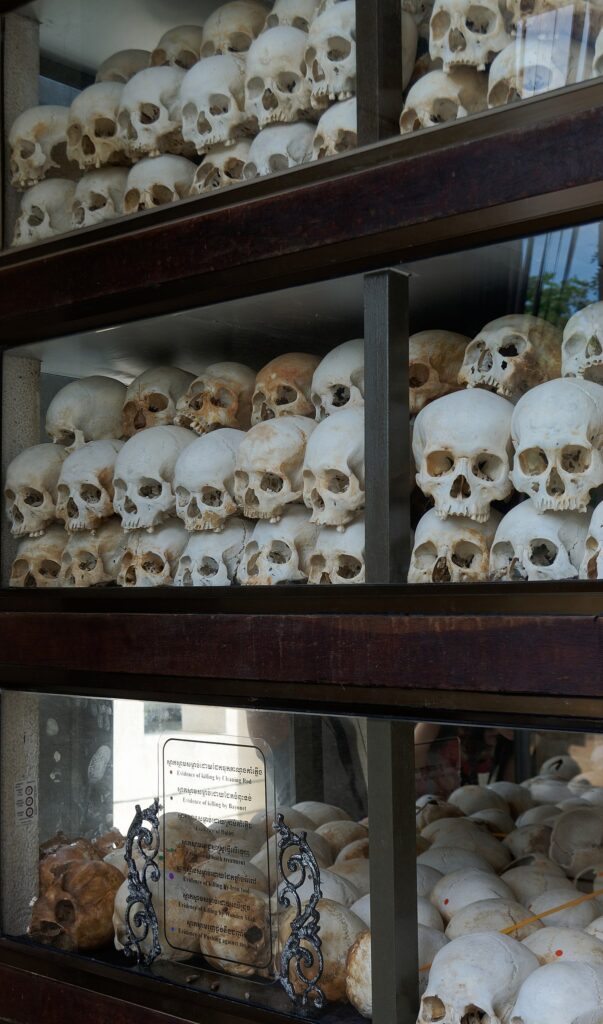
Jakub Hałun, Skulls at the stupa on the Choeung Ek Killing Field in Phnom Penh. Source: Wikimedia Commons
Anthropologist Hua Wu reports on the experiences of a group visiting the rural farm to which they were banished during China’s cultural revolution. Revisiting this site evoked various reactions in the participants. Caroline Bennett analyses haunting in Cambodia after the defeat of the Khmer Rouge by investigating how people re-established relationships with the death. The death remained a social presence, to which their surviving relatives reacted through funerary rituals and building shrines. It is exceedingly difficult to interpret these rituals as culturally specific expressions of psychological trauma.
Saiba Varma focuses on conditions in Kashmir, which is still occupied by the Indian army. Because the occupation is ongoing, Kashmiris are currently not post-trauma. Their trauma continues in the present; it is not relegated to the past. Seinenu Lemelson-Thein analyses the remarkable resilience of Myanmar’s freedom fighters, which is based on a cultural system of rites, rituals, and moral beliefs based on the concept of sacrifice (anitnah). Sadly, the situation in Myanmar has deteriorated dramatically over the past year.
In the final chapter, Maki Kimura describes how sculptures are used in the ongoing political battle of the so-called “comfort women,” women who were forced into sexual slavery by the Japanese Imperial forces during World War II. Japan still refuses to acknowledge the experiences of these women. By placing sculptures in strategic places, activists around the world highlight their plight.
We see discussions about trauma and PTSD as ways of dealing with violence and horror—or, at times, to obfuscate both. The case studies in this volume analyse both the psychological and communal effects of violence and natural disasters and how communities attempt to overcome their effects. At times, people in Asia incorporate and transform Western medicalised ideas, at other times transcend them and rely on local spiritual healing traditions, or even creatively combine both.
This volume transcends the traditional Western focus of trauma studies by highlighting Asia. We hope that this volume will inspire a shift in perspective for other scholars in this field.



{kind=link}